
The World Health Organization has just updated their Road Map for Neglected Tropical Disease (NTD) 2021-2030. This draft document was developed with stakeholders and outlines key actions for the control and elimination of NTDs including achieving the goal of schistosomiasis elimination as a public health problem (currently defined as less than 1% prevalence of heavy infections). While progress has been made towards schistosomiasis control targets, the new Road Map highlights the importance of extending current treatment activities to all those at risk of schistosomiasis.
An “age-ist” approach to schistosomiasis control
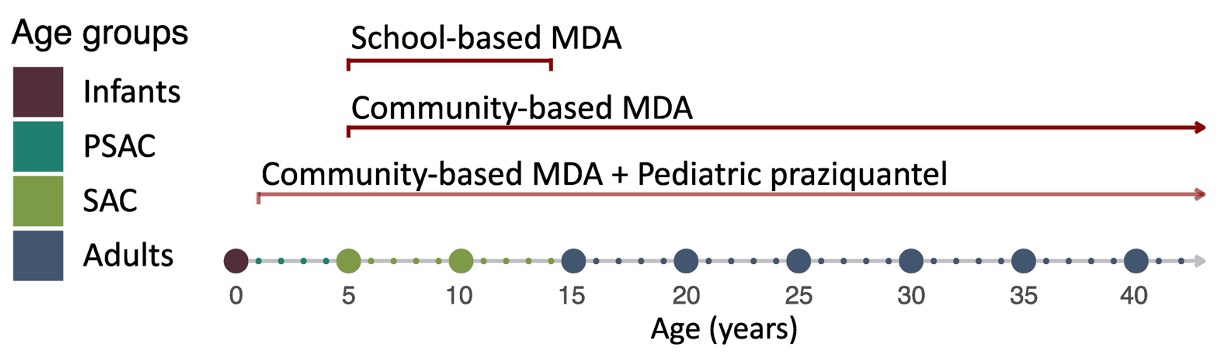
Typically, school-aged children (often abbreviated as SAC) are the focus of schistosomiasis control intervention programs, particularly in sub-Saharan Africa where approximately 90% of infections occur. These children are usually easy to access at primary schools for treatment (often referred to as school-based mass drug administration (MDA)), they often have high burdens of infection, suffer morbidity at key developmental stages and must be treated relatively frequently because they don’t yet have immunity and are rapidly (re)infected. School-aged children are the main demographic for monitoring, informing endemicity surveys, and intervention strategies.
It is clear that treating school-aged children is crucial, but individuals of all ages can get infected with, and suffer from, schistosomiasis. The focus on this age group for treatment and monitoring, has led to systematic interventions in a limited age group and leads to health inequity in other parts of the population. The current WHO treatment guidelines focuses on treatment intervention strategies based on SAC prevalence only and thus recommends community-wide MDA, i.e. including adults, if the prevalence in SAC is over 50% and treatment of special at-risk adult groups only if the prevalence in SAC is over 10%. But there is no inclusion of preschool-aged children (PSAC) in regular treatment programs.
Schistosomiasis Control Through the Ages
The Global Schistosomiasis Alliance organised a symposium at the European Congress on Tropical Medicine and International Health in Liverpool in September 2017. The symposium was called ‘Schistosomiasis Control Through the Ages” and brought together public health officials, epidemiologists, medical doctors, and other scientists to discuss how schistosomiasis affects individuals across all ages. This sparked a discussion that we recently published as an opinion piece.
Individuals in all age groups living in endemic communities can be susceptible to infections, but they face unique challenges for age-specific morbidity and treatment options.
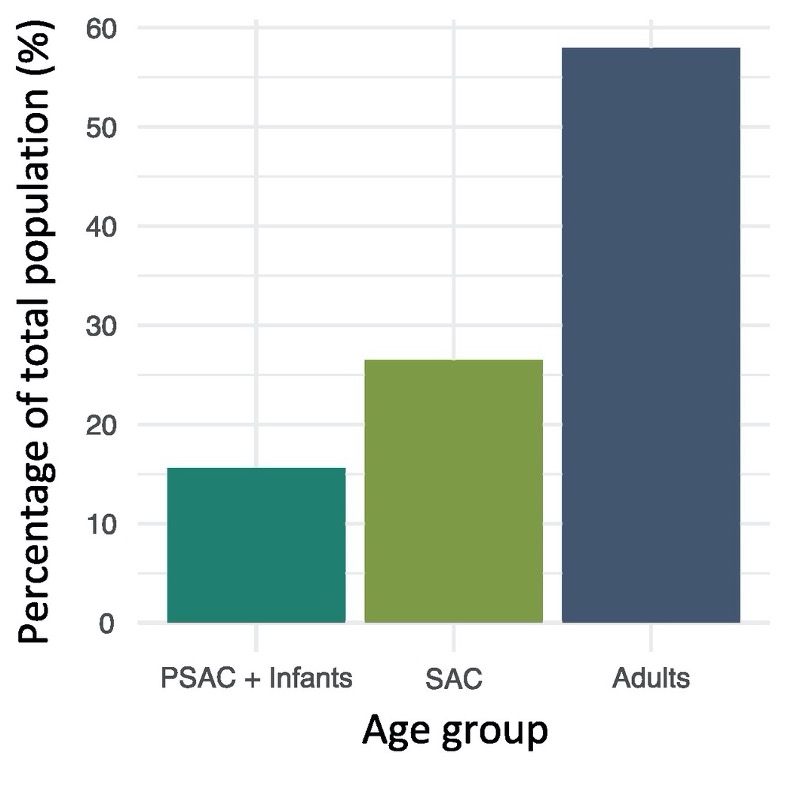
Key features of schistosomiasis and its control in preschool-aged children (around 15% of the population in sub-Saharan Africa):
- Praziquantel, the drug most effective against all schistosome species, is only licensed for ages of 4 years old and above.
- Most preschool aged children (1- 4 years of age) are not included in national control programmes.
- Children can have heavy infection intensities, and associated morbidities, at a very early age.
- Repeated treatments in this age group can reverse morbidity.
- Treatment with praziquantel can also enhance immunity to help reduce reinfection.
- A pediatric praziquantel formulation for 3 months and above is currently in clinical trials.
- Operational strategies and platforms to treat preschool-aged children are crucial to ensure this potentially high-risk age group is reached.
Key features of schistosomiasis and its control in adults:
- Treatment coverage is very low in adults – only 15% of adults needing preventive chemotherapy for schistosomiasis received treatment in 2018
- Adults can be away from the village or can’t leave work to get treated.
- Leaving a group of the population untreated can have significant impacts on bounceback of the disease in a community.
- It is safe to use praziquantel during pregnancy and lactation, but treatment of pregnant and/or lactating women is often not implemented in programs.
- Infection with schistosomiasis can lead to genital manifestations of the disease, which are often underreported due to stigma, and/or misdiagnosed by health services.
- Sensitive diagnostics are urgently needed for diagnosing female genital schistosomiasis (FGS) and male genital schistosomiasis (MGS).
- Early treatment with praziquantel can reverse some pathology, but more research is needed to address chronic and severe morbidities in adults.
Closing the gap: equitable treatment interventions and access
The NTD Road Map has identified extending praziquantel treatment to all those at risk as a high priority. This will require an increase in the amount of praziquantel available for MDA, the deployment of pediatric formulations and, increased access to treatment through age and demographic appropriate platforms. Achieving elimination of schistosomiasis as a public health problem in all countries by 2030 will not only require extending treatment to all at-risk individuals, but also integrating vector control, education and water, hygiene and sanitation interventions.


Comments