As a medical doctor working in my home country of Malawi, I have seen the detrimental impact of many Neglected Tropical Diseases (NTDs) in our hospitals as well as on-the-ground in field-based clinics. NTDs comprise of 23 principally communicable diseases, prevalent in low- and middle-income countries, typically within tropical and sub-tropical environments. Over 1 billion people are affected by at least one NTD, and collectively these NTDs contribute to a substantial morbidity and disability burden globally, entrapping many in poverty.
My PhD focus is on the epidemiology and pathology of schistosomiasis, specifically Male Genital Schistosomiasis (MGS) in fishermen along the shoreline of Lake Malawi. I have recently published a systematic literature review on the clinico-pathological features associated with MGS, highlighting a possible connection of the disease with HIV infection (also presented at 2018 International Congress of Parasitology). Our major findings were that 1) current diagnostics for epidemiological surveillance of MGS need to be improved; 2) infections are under reported and the burden is underestimated; and 3) HIV co-infection needs to be considered when optimising individual case management and reviewing Praziquantel dosing regimens.
Background
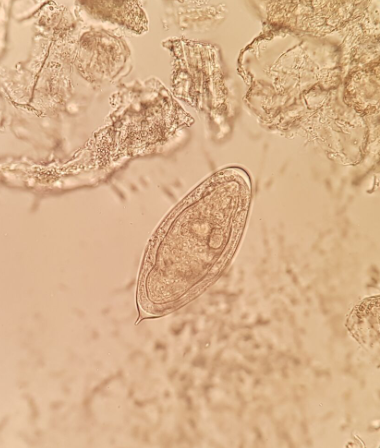
Globally over 200 million people suffer from schistosomiasis every year, with over 90% of infections occurring in sub-Saharan Africa (SSA). As described in previous Bugbitten blogs, this snail-borne disease is predominantly caused by two species of schistosome flukes; Schistosoma haematobium and Schistosoma mansoni, responsible for urogenital or intestinal disease respectively. The infection is contracted when people come into contact with contaminated waters, during routine household, recreational, agricultural and income-generating activities in their communities. Despite efforts, accurate diagnosis of these blood vessel-dwelling flukes, the various species and the different life-cycle stages- remains a challenge.
MGS, described as the presence of schistosome eggs in semen or associated pathologies from entrapped eggs in male genital organs, causes various symptoms including spontaneous pelvic or ejaculatory pain, haemospermia, ejaculate irregularities, erectile dysfunction, infertility, enlarged genital organs, as well as histopathological and radiological abnormalities. Despite these horrific symptoms, MGS awareness is scarce even in endemic areas and many clinicians overlook the genital-associated complications of schistosomiasis, thereby affecting downstream diagnosis and treatment.
Fieldwork in Malawi
As part of my PhD, I set out to investigate the prevalence and morbidity of MGS in an endemic area. We set up a longitudinal cohort study among fishermen on the shoreline of Lake Malawi, Mangochi District from November 2017 to December 2018.
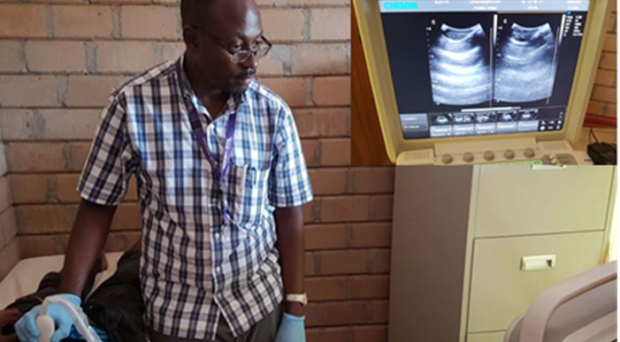
Due to the challenging nature of collecting semen samples from participants, the first challenge was defining our methodologies for ethical review. After much discussion, an effective communication plan and pre-study sensitisation strategy was finalised in the hope that compliance would be as high as possible. 376 fishermen were recruited and interviewed using a standardised questionnaire. Mid-morning urine, semen and blood samples were collected for both field diagnosis of S. haematobium and further molecular analyses at the Liverpool School of Tropical Medicine, United Kingdom. Transabdominal and scrotal ultrasonography were also employed to investigate any genital pathologies. Subsequent praziquantel therapy was offered to participants, along with an invitation to follow-up studies at 1, 3, 6 and 12 months.

Preliminary results
Of the 210 participants who submitted urine at baseline, 17.1% had S. haematobium egg-patent infections. Astonishingly, the presence of schistosome eggs in semen samples was confirmed in 10.7% of the 112 participants who provided semen samples. Of those, one third also had eggs in their urine. A fifth of the participants who underwent transabdominal and scrotal ultrasonography, had pathologies in the prostrate, seminal vesicles and testes. At the 1-month follow-up after praziquantel therapy, prevalence of urine egg-patent infection reduced to 11.1%, and no eggs were seen in the submitted semen. Further molecular analyses are underway to further investigate MGS characteristics of these samples. Excitingly, the full results will be presented at the Spring Meeting of the British Society for Parasitology and published soon after.
Given the disease has been overlooked for so long, I was surprised by these initial results- especially the high prevalence of MGS amongst the fishermen and other people exposed to the infectious water bodies in Malawi! Encouragingly, these preliminary results indicate that the current treatment can clear the MGS infections. Unfortunately, in many areas of Sub-Saharan Africa where access to diagnostics and treatment is limited, urogenital schistosomiasis (caused by S. haematobium) is endemic and millions of men suffer unduly from MGS. I would like to see that my research efforts are playing an influential role in raising greater awareness and surveillance as well as positively influencing better case management of men with MGS.
Comments