What do you do?
I map infectious diseases and their vectors, the organisms that spread them. I’ve worked on the Malaria Atlas Project, which looks at the global distribution of malaria and how that changes in relation to interventions across the world.
More recently, working on influenza outbreaks in China and Ebola in Africa, we’ve been looking at quicker mapping techniques that can help in emergencies. This means that when a novel pathogen (a thing that causes disease, such as a bacteria strain or a virus) comes out, we can quickly find the areas in which it, and perhaps its insect vectors, can survive and flourish, based on things like temperature, rainfall and habitat.
How are these maps used?
Most obviously they can help show where the biggest problems might be and help people focus surveillance activities. Mapping can also help inform travel advisories, showing the places where people might want to take extra precautions if they visit.
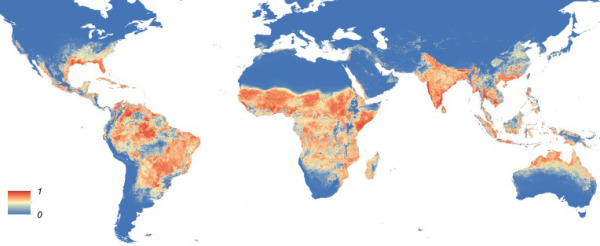
Assuming a virus is easily moved around the world by people on aeroplanes, we can also show all the parts of the world that could ultimately end up with infections because they are environmentally suitable.
Are you mapping Zika virus?
Yes, we’re in the midst of trying to put together a global suitability map for Zika. We have done some previous work looking at the global distribution of dengue and chikungunya, which are related viruses, so we’re in quite a good place to make these maps.
How easy is it to predict what the next big epidemic will be?
Up until mid-2014, Zika was just one of tens of related viruses and hundreds of things a non-clinician like me would find in the appendix of a book on infectious diseases, most of which you’ve never heard of.
The only thing we can say with certainty is that these things will continue to happen. Up until mid-2014, Zika was just one of tens of related viruses and hundreds of things a non-clinician like me would find in the appendix of a book on infectious diseases, most of which you’ve never heard of. It’s not always an issue of new bugs appearing, but of one of many known things emerging in different places for whatever reason.
I would have a great deal of scepticism about anybody who told me they could predict the next pandemic. That doesn’t mean science is bankrupt. We know there are probably areas that are more or less predisposed, so it’s a bit like long-term climate forecasting.
We can say there are higher probabilities in some parts of the world than there are in others, but the idea you can go from that to saying ‘It’s going to be this particular pathogen, on this date, in this village’ is highly unlikely.
How can we ensure responses to epidemics are proportionate?
That’s a really tricky one. If I’m a public health authority or a politician that has invested an awful lot of money in a disease or epidemic that doesn’t eventually take hold, then I’m criticized for having wasted money. If I don’t invest that money and the disease takes hold, then I’m equally criticized. The wider community has to step back a bit and ask what success is in this domain. How do we genuinely hold people to account?
We need to be able to respond to these things quickly, and I think most people in most countries would expect those involved in determining their public health policy to be able to do that. Sustaining the ongoing costs of this is clearly another central challenge.
How do we best prepare given the uncertainty?
In terms of what I do, I think we have to get systems and processes in place so that when something new emerges we can get the information we need rapidly.
In terms of what I do, I think we have to get systems and processes in place so that when something new emerges we can get the information we need rapidly. This means being able to mobilize people to make the maps and get them to those that need them as quickly as possible, and then to keep the maps up to date.
The big problem is how we maintain our ability to respond to these outbreaks when we’re not in the midst of one. I think the trick is to try and blur the boundaries between epidemic response and routine healthcare so they’re not viewed as one taking resources from the other.
If we can work out how the resources you need to rapidly mobilize in emergencies can be usefully deployed for more routine things, epidemic response can become more sustainable.
What’s the one change you’d make in the world to make us better prepared for epidemics?
It would be some mechanism whereby people can share information as quickly and as openly as possible. I’m not a frontline clinician dealing with the hard end of this business, but time and time again I see bureaucratic obstacles to sharing in emergencies – affecting everything from the genomes of pathogens to patient data.
I think that some progress has been made, but getting improved mechanisms and agreements in place so that all of these things are streamlined in emergencies would put us in a much better place to get more hands on deck quicker.
Comments