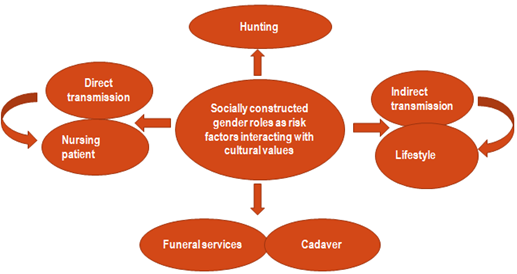
The circle of interacting risk factors provides insight between Ebola risk factors and socially constructed gender roles interacting with cultural values. It provides an insight into the link between gender and the risk of contracting infectious diseases using Ebola virus in African context.
Recently, the concept of gender and sex has been given global attention in research. These two concepts are inter-related: Sex denotes biological differences; gender refers to the socially constructed roles which vary from one society to another.
Bush meat
From observation, all known sources of the index cases of Ebola virus disease since 1976 have been traced to either exposure and/or hunting of wild animals (chimpanzee, monkeys, gorillas etc.) in the rain forest.
In the African context, these wild animals are referred to as “bushmeat”. Bush meat is a source of protein and is also considered a source of income and livelihood in most rural African families. Moreover, the consumption of bush meat is not linked to differences in socio-economic status in Africa.
Hunting of bush meat is an occupation and an activity that is culturally associated with men within the African context. This increases men’s exposure to contracting Ebola virus.
Hunting of bush meat is an occupation and an activity that is culturally associated with men within the African context. This increases men’s exposure to contracting Ebola virus which can be attributed to time spent away from home and responsibility for caring for livestock.
Gender roles
In the African context, women are considered as primary caregivers at home. In contrast, it is uncommon for men to take care of their wives or children when they are ill. This increases the level of exposure of women to contracting the virus.
Transmission of Ebola virus has been found to be higher in homes than in hospital. It is important to note that direct transmission of Ebola virus occurs through contact with infected patients’ bodily fluids or dead bodies. Indirect transmission may occur when sharing meals, washing clothes, sharing clothing, sleeping in the same bed, shaking hands, or hugging. Both men and women also have specific cultural roles to perform during funeral services. All these risk factors and related exposures interact with cultural values and practices creating a circle of interacting risk factors.
As an African, over the years, I have come to terms that African women take on the role of “nurses” in their homes. This is because as caregivers, they perform the task that to some extent, are similar to those tasks performed by nurses in the hospital. However, nurses are trained and accredited, unlike the informal caregivers. The question is: do we take into consideration these informal caregivers when designing health programs in a specific context? The Liberian case provides more insight to this.
Communicating risk
Considering that Ebola is a risk, and the onset of the outbreak has been perceived by the community as either a “mysterious illness” or “witchcraft”. Effective risk communication takes precedence especially as there is not yet any licensed treatment.
Just as risk perception varies by context, gender, and level of education, all of which may also influence care-seeking behaviour. Knowledge and access to health services equally vary by gender in the African context.
The public health messaging during the 2014 Ebola outbreak emphasized that “Ebola is real”, with repeated messages that “it is deadly and has no cure, no treatment, and no vaccine”. Such messages may lead to differences in processing and understanding of the risk, especially when technical or scientific terms are used, such as “no cure, no treatment, and no vaccine”, in addressing a lay population with multiple spoken languages and dialects.
Moreover, gender differences in the use of services may arise depending on several factors: To whom and in what language is the message actually delivered? Who actually makes the decision to seek care and who actually cares for the patient?
Given that not all risk can be managed at the domestic level and because risk assessment informs subsequent risk management, the hope is that, this scoping review published in Infectious Diseases of Poverty will add and provide insight to health planners in understanding and respecting subtle cultural and socio-economic undertones relating to gender within a specific context and to build the capacity for effective risk communication as a worthwhile investment for both local and global public health authorities.
Comments