Every year, globally, around $270 billion is invested in biomedical and health research. But is it worth it?
This may be a facile question to some – clearly it is worth it: average life expectancy in England is expected to rise to the late 80’s by 2030 , cancer survival rates in developed countries are improving, and a number of killer infectious diseases – such as polio – are on the verge of being wiped out.
But these emotive arguments have limited traction with those who hold the purse strings in finance ministries. They would point out that $270b could be invested elsewhere – on improving schooling for kids, on investing in social care for the elderly, on strengthening national security, or on building new roads and rail systems.
To counter these rational arguments, and make the case for research, it is important to speak the language of finance by estimating the economic returns from research.
In a series of papers, the last of which was recently published in Health Research Policy and Systems, we have attempted to estimate the economic returns from biomedical and health research. We analyzed two major elements: the monetized health gains from the UK application of relevant UK research, and the broader impact on the UK Gross Domestic Product (GDP).
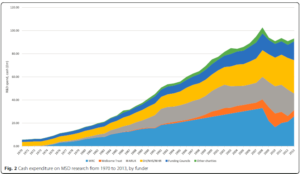
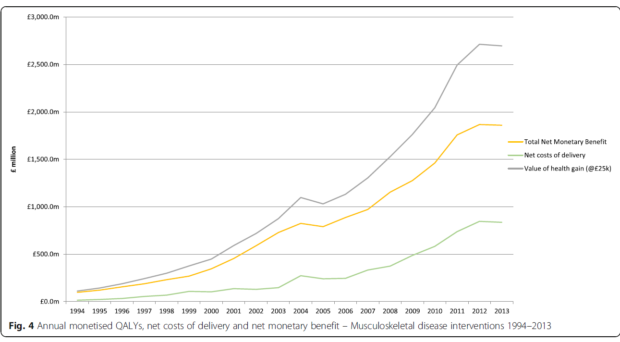
To assess the return in terms of health gains, we first estimated the amount of public (government and charity) money spent on research in three different areas – cardiovascular disease (CVD), cancer and musculoskeletal disease (MSD). We then estimated the elapsed time between the research investment and the net monetary benefits (NMB) arising from the research. This was calculated as the net monetary value of the health gain that should be attributed to the national research investment, minus the cost of delivering that health benefit for a list of key research-based clinical interventions.
This health benefit arising from biomedical and health research was measured and monetarized through Quality Adjusted Life Years (QALYs). A QALY is a measure of the health of a person or population which incorporates both length of life and the quality of that life, so one QALY is equal to 1 year of life in full health. We valued QALYs based on an estimate of how much it costs the UK National Health Service (NHS) to generate an extra QALY (with a base case of £25k).
Using these four key elements of data, we could then attribute a proportion of the annual NMB of the health gain as being due to UK research, and relate an equal number of years of investment to years of NMB, ‘lagged’ by an estimate of the average time between research and benefit. The return is expressed as an internal rate of return (IRR), which is effectively the discount rate that would yield a zero net present value. For CVD research this produced a best-case estimate of 9%, and when this approach was applied to cancer research and MSD research the respective IRR was 10% and 7%.
In a fourth paper we estimated the economic ‘spillover’ effects. The term ‘spillover’ is used by economists to describe an investment by one organization, public or private, that benefits other organizations in both the same and different sectors of the economy. For example, the decision by AstraZeneca to establish its global HQ in Cambridge, UK, has an economic impact on Cambridge. The investment is creating new jobs, increasing the demand for housing, encouraging other companies to co-locate, and so on.
By looking at the relationship between public and private R&D investment (in economic terms, the elasticity), it was possible to show that every additional £1 of public spend on biomedical and health research is associated with an additional 99p of private R&D spend in the UK. By combining the estimated elasticity with previous estimates of the social rate of return from private R&D spend of around 50%, the best estimate IRR, in terms of impact on GDP of public biomedical and health research spend, was between 15% and 18%.
Added to the estimates of the NMB of health gains arising from research, this would suggest a total return to CVD, cancer and MSD research of around 25% (i.e. around 10% for the health gains plus approximately 15% for the GDP gain). This means that for every one pound spent on medical research in the UK, we get back benefits, in GDP gains and health gains, equivalent to 25p per year. Comparisons with other public sectors are difficult due to different methodological approaches and lack of studies in other areas, but these figures are well in excess of the yields of 6-8% that governments typically expect from public investments.
It should be stressed that numerous assumptions are inevitably made in coming up with these estimates (as documented in the papers) and that they reflect past performance and are no guarantee of similar future returns.
But those caveats aside, our work suggests that, to put it simply, public investment in biomedical and health research returns an impressive bang for your buck.
Comments