What are the benefits of biomedical and health research? This is the core question at the heart of any decision to fund research – whether made by the government on behalf of taxpayers or medical research charities on behalf of donors.
But at the same time it is a methodologically challenging question – there are a set of perennial issues, such as the time it takes for research to move from bench to bedside, benefits arising from many different research projects, and the vexing issue of measuring and actually valuing research.
In the past our group and colleagues have published two studies that have attempted to measure the economic returns from publicly (government and charitable) funded biomedical and health research in the UK for two areas –cardiovascular disease and cancer.
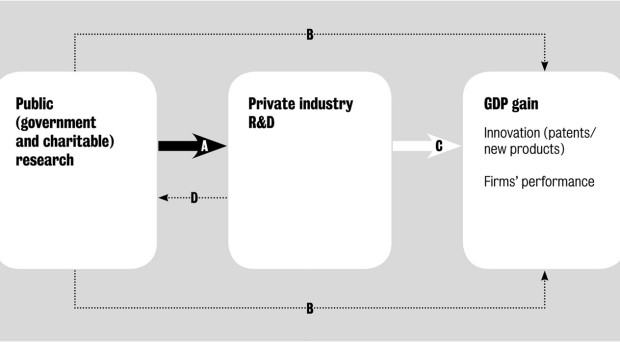
For both studies we identified two types of impact. The first is health gain, that is, the (net) monetised health benefit of living longer and healthier lives. The second is ‘GDP gain’, that is, the benefit to the wider economy arising from public and consequential private sector biomedical and health research activity, including additional private sector research and development (R&D) spending.
Much of the economic gain from public biomedical and health research is achieved by stimulating additional private industry R&D. Such ‘spillovers’ from public to private research are often a deliberate policy objective of spending on public research.
At its simplest, the monetised health benefit is estimated by collating the amount of research money invested into a disease area over time and relating that to the health gain as measured through quality adjusted life years (QALYs).
The relationship between the inputs (money) and outcomes (health gain) are adjusted for estimates of the amount of time it takes for research to translate to improvements in health and for the amount of the health gain that can be attributed to UK research (as opposed to research from other countries).
By relating these four pieces of information we estimated that the health benefit rate of return (RoR) was 9% for cardiovascular research and 10% for cancer research. To get an overall estimate of the RoR to public research you then have to add these health gain estimates to the effect on GDP.
‘Spillover’ effect
In previous studies we had relied on other peoples’ research from the USA and came up with a rate of return as measured by GDP of 30%, which is additional to the 9%-10% return achieved in terms of health gain. This 30% estimate was arrived at by looking at how much private sector research investments are influenced by public sector research funding, and then multiplying that additional funding by estimates from the literature of the social rate of return to private R&D.
In a recent paper published in BMC Medicine we have developed an up to date estimate and one that is specific to the UK, for the extent of public/private spillovers in biomedical and health research.
We were interested in investigating whether public and private sector research ‘complement’ each other or are ‘substitutes’.
Complementarity is when investments in one sector stimulate activity in another sector; substitution occurs when investment in one sector replaces activity in the other.
We fitted an econometric model to time series for biomedical and health R&D expenditure in the UK for ten disease areas (including ‘other’) for the public and private sectors respectively.
We found that there was a statistically significant complementary relationship between public (government plus charity) biomedical and health research expenditure and private pharmaceutical R&D expenditure in the UK.
Economic impact
A 1% increase in public sector expenditure is associated in the best-fit model with a 0.81% increase in private sector expenditure. With that magnitude of relationship, every additional £1 of public research expenditure is associated with an additional £0.99 of private sector R&D spend in the UK; 44% of that additional private sector expenditure occurs within one year, with the remainder accumulating over decades.
Using these new estimates we could then re-estimate the total impact of biomedical and health research in the UK on the UK economy, by using the same estimate as in the earlier study of the social rate of return to private R&D.
This implies a real annual rate of return (in terms of GDP impact) to public biomedical and health research in the UK of around 17% (as opposed to our earlier figure of around 30%).
We should stress this does not imply that there has been a decline in the economic rate of return to public spending on biomedical and health research – what we have developed in this paper is a contemporary estimate based for the UK specifically.
Indeed, when combined with the net health benefit (of c10%) the total return on government and charitable research investment in the UK is around 27% – a significant return on investment in anyone’s book.
Comments