It is now well established that different human populations may exhibit very different responses to therapeutic drugs. However, to what extent this may have been influenced by our evolutionary history is less well known. In this guest blog, Ripudaman K Bains from University College London outlines why understanding our past can help inform our future, and describes her recent work published in BMC Genetics with colleagues from Addis Ababa University, Henry Stewart Group and Uppsala University on molecular diversity and population structure at the Cytochrome P450 3A5 gene in Africa.
 One of the most significant accomplishments of the genomics revolution has been an improvement in our understanding of why certain populations have elevated risks for developing specific diseases. It has enabled us to examine diversity across multiple and previously uncharacterized human populations and improved our understanding of human genetic diversity across geographic regions, ultimately helping us to identify the evolutionary processes that have shaped population differences. There are now well-established ethnic and population differences in the genetic predisposition to certain diseases; for example the higher risk of Tay-Sachs disease in Ashkenazi Jewish populations (1, 2) and the high proportion of blood disorders in populations from malaria endemic regions, such as glucose-6-phosphate dehydrogenase deficiency (3) and sickle cell disorder (4, 5).
One of the most significant accomplishments of the genomics revolution has been an improvement in our understanding of why certain populations have elevated risks for developing specific diseases. It has enabled us to examine diversity across multiple and previously uncharacterized human populations and improved our understanding of human genetic diversity across geographic regions, ultimately helping us to identify the evolutionary processes that have shaped population differences. There are now well-established ethnic and population differences in the genetic predisposition to certain diseases; for example the higher risk of Tay-Sachs disease in Ashkenazi Jewish populations (1, 2) and the high proportion of blood disorders in populations from malaria endemic regions, such as glucose-6-phosphate dehydrogenase deficiency (3) and sickle cell disorder (4, 5).
Genetic variability does not only influence disease phenotype and pathology; it can also influence the safety and efficacy of drug treatment. As such, the results of drug therapy can vary within and between populations. Most patients respond well to drug treatment at standardized dosages, however there are individuals who have minimal or no therapeutic response. Additionally, some patients experience severe adverse drug reactions, which are major contributors to global morbidity and mortality. Once a drug is administered, it is absorbed and distributed to the site of action, where it interacts with targets such as receptors or enzymes. Most drugs undergo metabolism before being excreted. Genetic variation may affect absorption, enzyme activity, cellular uptake, and metabolism, resulting in altered drug activity or half-life. Variation in genes encoding drug metabolizing enzymes, such as those in the Cytochrome P450 (CYP450) super-family, can contribute to sub-optimal clinical outcomes.
Tailored therapy
The clinical vision for studies of genes encoding drug metabolizing enzymes is that genetic variation identified within these genes may one day be used to tailor drug therapies based on an individual’s genotype. However, the implementation of genotype-guided medicine for individuals is not currently in widespread clinical use. Physicians are becoming increasingly aware of clinically relevant genetic polymorphisms. However, a 2006 study by the Federal Drug Administration reported that only ~25% of all prescriptions written in the USA contained pharmacogenetics labeling. The paucity of affordable and efficient testing methods, in addition to the continuous identification of clinically important genetic variants, has delayed the translation of human genetic information into clinical practice and healthcare administration. Population-based studies can go some way towards filling this gap. Studying the distribution of pharmacogenetically relevant variants among populations, instead of individuals, has identified common, medically important, variation. However there are many populations, particularly within Africa, that remain under-represented in population pharmacogenetics studies.
The importance of including African populations within evolutionary and clinical research should not be underestimated. The majority of archaeological and genetic data support a recent African origin model of the evolution of anatomically modern humans ~150,000-200,000 years ago. As a result Africa has extensive inter-ethnic genetic diversity, in addition to considerable inter-ethnic cultural, phenotypic and linguistic differences. From a medical perspective, there are marked differences between African populations and European populations in the response to specific treatments that are administered for diseases. However, over 95% of drug development and clinical trials are carried out in European and North American populations, both with predominantly recent European ancestry. Many developing countries, including those in Africa, rely on FDA and European guidelines for safety levels and optimal therapeutic dosages. There are few large-scale studies examining variation in drug metabolizing enzymes across multiple, geographically and ethnically diverse African populations.
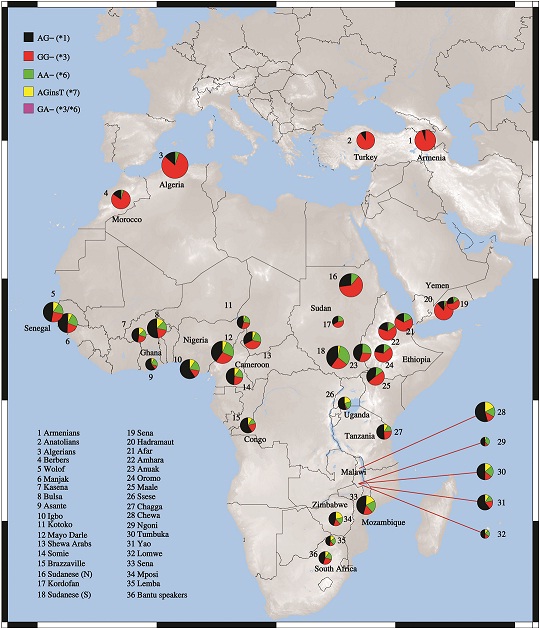
In our recent BMC Genetics publication we attempted to address this imbalance. We used a multi-disciplinary approach to characterize and analyze intra-African variation at the gene encoding the drug metabolizing enzyme Cytochrome P450 3A5 (CYP3A5), which is involved in the metabolism of ~50% of all clinically administered drugs. However, CYP3A5 is variably expressed; individuals tend to express the protein at high concentrations or have low to undetectable levels of protein. In addition to being the largest study, to date, of CYP3A5 variation in Africa, our approach differs from previous studies in that we used molecular and evolutionary approaches to understand population-level variation in the CYP3A5 gene. Our study found that CYP3A5 is likely to be one of the most pharmacologically active drug metabolizing enzymes in Africa. Our estimate of the proportion of individuals across Africa who express CYP3A5 (43%) is considerably lower than previous, independent estimates from the continent (55-95%). This is considerably higher than independent estimates for individuals with recent European ancestry (10%), Asian (25%) and South American (30%) populations. Our findings suggest that there are likely to be multiple pharmacogenetics profiles, relating to variable CYP3A5 expression, across different African populations.
Evolutionary medicine
 We also examined population differences in the frequencies of functional variation at the CYP3A5 gene in an evolutionary context. CYP450 genes are largely studied for their role in drug and hormone metabolism. However, the ability of these enzymes to metabolize drugs is a by-product of what is believed to be their “native” role, since CYP450 paralogues exist in multiple prokaryotic and eukaryotic species, and the genes are thought to have existed on the planet for over 2 billion years. It is thought that the ability of CYP450 enzymes to metabolize exogenous compounds evolved 400-500 million years ago to enable animals to digest certain toxic chemicals found in plants, creating water-soluble compounds which are easier to excrete. Their role as drug metabolizing enzymes has arrived very late in human evolutionary history.
We also examined population differences in the frequencies of functional variation at the CYP3A5 gene in an evolutionary context. CYP450 genes are largely studied for their role in drug and hormone metabolism. However, the ability of these enzymes to metabolize drugs is a by-product of what is believed to be their “native” role, since CYP450 paralogues exist in multiple prokaryotic and eukaryotic species, and the genes are thought to have existed on the planet for over 2 billion years. It is thought that the ability of CYP450 enzymes to metabolize exogenous compounds evolved 400-500 million years ago to enable animals to digest certain toxic chemicals found in plants, creating water-soluble compounds which are easier to excrete. Their role as drug metabolizing enzymes has arrived very late in human evolutionary history.
The application of evolutionary principles to medical research – the emerging field of “evolutionary medicine” – attempts to understand how environmental and genetic factors have shaped our vulnerabilities and responses to diseases and therapies throughout human evolutionary history. We attempted to identify environmental factors which may predict CYP3A5 expression patterns across global regions, and infer evolutionary factors which may have shaped the observed correlations. CYP3A5 is involved in the metabolism of renal cortisol to 6-β-hydroxycortisol, a key regulator of renal sodium transport. From an evolutionary perspective, salt and water retention are vital traits in populations that frequently experience water shortages. A previous study reported that equatorial populations, which are most vulnerable to water shortages, were much more likely to express CYP3A5 at high concentrations. Within these regions, rapid salt and water retention should provide an evolutionary advantage.
We examined this further by testing for correlations between CYP3A5 expression phenotypes and ecological data relating to aridity for the present day, the Holocene (the last ~10,000 years) and the Late Pleistocene (~50,000 to ~10,000 years ago) periods. We found significant gene-environment interactions, which show that individuals living in dry and arid environments are more likely to express CYP3A5. Interestingly, we found significant correlations between high CYP3A5 expression phenotypes and aridity data from the Holocene and Late Pleistocene. This was also seen for temperature data for each time period. Our findings provide further support for a hypothesis that the CYP3A5 enzyme may have been involved in salt retention and heat adaptation, which explains some of the differences in CYP3A5 expression patterns that we observed across Africa.
There remains a need for focused studies to establish the relationship between environmental variables, patterns of genetic variation, and clinical outcomes within Africa. This is not limited to studies of CYP450 genes; detailed studies of additional drug metabolizing genes, and genetic markers important in predicting clinical outcomes, will become increasingly necessary as we move towards the era of personalized genomics.
1. Myerowitz R; The search for the genetic lesion in Ashkenazi Jews with Classic Tay-Sachs disease. Adv Genet 2001;44:137-43.
2. Frisch A, Colombo R, Michaelovsky E, et al.; Origin and spread of the 1278insTATC mutation causing Tay-Sachs disease in Ashkenazi Jews: genetic drift as a robust and parsimonious hypothesis. Hum Genet 2004;114(4):366-76. doi: 10.1007/s00439-003-1072-8.
3. Tishkoff SA, Varkonyi R, Cahinhinan N, et al.; Haplotype diversity and linkage disequilibrium at human G6PD: recent origin of alleles that confer malarial resistance. Science 2001;293(5529):455-62. doi: 10.1126/science.1061573
4. Mabayoje JO; Sickle-cell anaemia; a major disease in West Africa. Br Med J 1956;1(4960):194-6.
5. Trowell HC, Raper AB, Welbourn HF; The natural history of homozygous sickle-cell anaemia in Central Africa. Q J Med 1957;26(104):401-22.
Explore more on developments in evolutionary medicine in this article collection from BMC Medicine: Evolutionary Medicine : clinical medicine from an evolutionary perspective
[…] Variability in the gene encoding the drug metabolizing enzyme Cytochrome P450 3A5 (CYP3A5) from 36 ethnically diverse populations in Africa reveals that 43% of individuals express this gene, consistent with it playing a role in salt-retention. Lead author of the study Ripudaman K Bains from University College London outlines how understanding our evolutionary past could help guide drug therapies of the future. […]