Thrombosis – blood clots that form in an artery or vein – is the one disorder that causes all three of the world’s top cardiovascular killers: heart attack, stroke and venous thromboembolism (VTE). Today is World Thrombosis Day, and to mark it, the Editors of Thrombosis Journal have put together some of the key things you ought to know about thrombosis and the associated risks.
An estimated 17.3 million people die every year from cardiovascular disease, making it the number one cause of deaths globally. This is estimated to increase to 20.3 million deaths by 2030. Given these numbers, it is undoubtedly vitally important for us to understand the mechanisms and causes of these diseases.
Heart attacks and strokes are, for a major part, related to atherosclerosis, where arteries become clogged up by fatty substances known as plaques or atheroma. This is the final result of commonly acquired risk factors including high blood pressure, high cholesterol, smoking, obesity and diabetes. It’s often linked to the “western lifestyle” but is becoming increasingly common in other areas of the world.
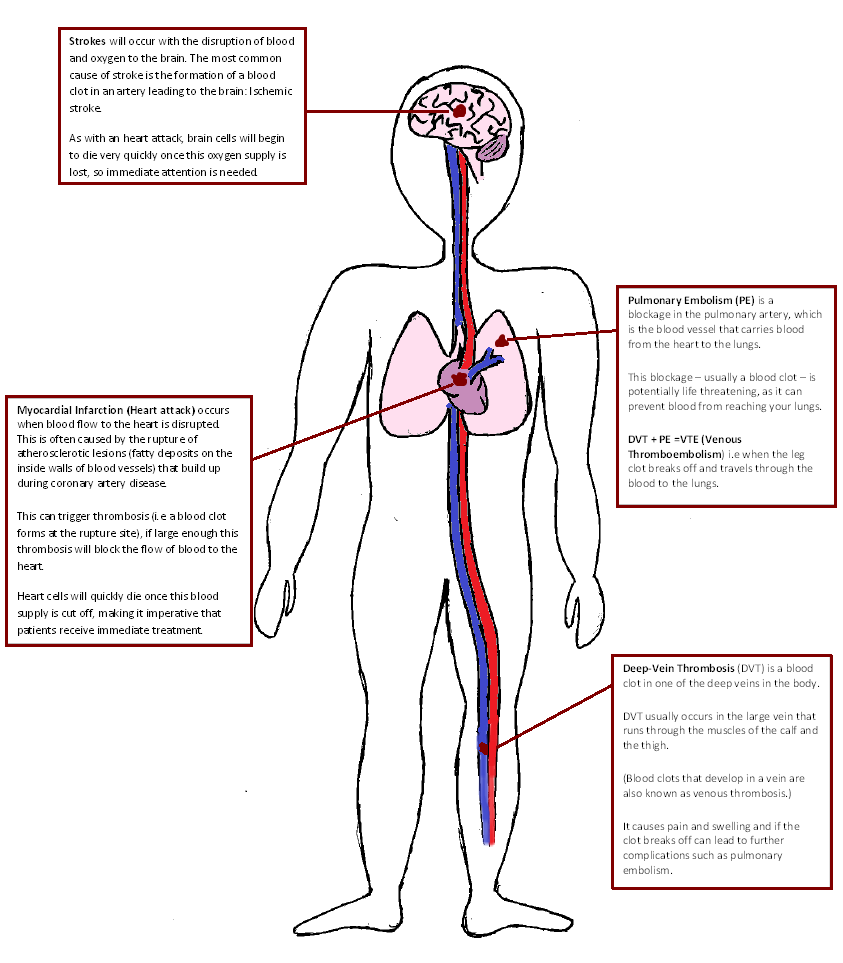
When atherosclerotic lesions in blood vessels providing the heart or brain with oxygen and nutrients rupture, they trigger thrombosis. This prohibits blood flow to the heart or brain, resulting in a heart attack or stroke.
A major part of ischemic strokes are, however, linked to another related illness, atrial fibrillation. This heart rhythm abnormality can cause thromboembolism in the left atrium, which may migrate to the brain.
Finally, the most important theme of this year’s WTD is venous throemboembolism, occurring in 1:1000 individuals on average, a potentially fatal disease (due to pulmonary embolism) with a number of complications, including post thrombotic syndrome.
Having an understanding of thrombosis and its causes is key in helping us to tackle cardiovascular diseases. So here are some of the key things you should be aware of:
1) Deep vein thrombosis can kill.
When a blood clot forms in a deep vein (mostly in the leg), this is called a “deep vein thrombosis” or DVT. This clot can break off and travel to other areas of the body. If the clot breaks off and travels from the leg up to the lungs, it can block the artery leading into the lungs, causing a pulmonary embolism (PE).
Together, DVT and PE are known as venous thromboembolism (VTE), which contributes to half a million deaths in Europe alone (more than the combined totals of AIDS, breast and prostate cancers and road traffic accidents!).
2) Thrombosis affects seemingly healthy people of all ages.
Although more prevalent at a higher age, it does not just affect the overweight and elderly. Many cases are seen in young, seemingly fit people. A prime example of this is tennis champion Serena Williams, who suffered a pulmonary embolism in 2011, possibly as a result of foot-surgery that she underwent. Luckily the clot was discovered before it could cause any lasting damage.
3) Not everyone experiences symptoms.
However there are warning signs and these vary depending on the position of the clot:
-Deep vein thrombosis: pain or tenderness (usually starts in the calf), swelling including the foot and ankle, redness or discoloration, warmth.
-Pulmonary embolism: unexplained shortness of breath, rapid breathing, chest pain (may be worse with deep breath), rapid heart rate, light headedness/fainting. While these are common signs for many other conditions, they may be symptoms of PE if you have related risk factors.
4) It is possible to lessen the risk.
If a doctor considers a patient to be at risk they can prescribe anticoagulants and/or platelet inhibitors. Many groups are developing tests to analyse patient risk. For instance this study by Tamura et al looks at the Global Thrombosis Test for assessing patient risk for those undergoing total knee arthroplasty.
5) New oral anticoagulants are changing treatment.
These agents, now referred to as non-vitamin K dependent oral anticoagulants (NOACs) are different from the routinely used vitamin K dependent anticoagulants (VKAs). The introduction of the NOACs in daily practice is not much less than a revolution in antithrombotic management, since they appear to provide a simpler, effective and, in some aspects, even safer form of anticoagulation. Tahir et al systematically review the phase three clinical trials of new oral anticoagulants in common medical conditions in this manuscript.
However, several hurdles need to be overcome before NOACs can replace VKA as the main form of oral anticoagulation; these include more insight into long term effects and possible side effects, availability of specific antidotes and availability of laboratory techniques to control blood levels of NOACs, as described in this review by Hugo ten Cate.
Finally, as the NOACs do not require regular laboratory monitoring and dose adjustment (as is the case with warfarin, one of the best known VKAs), there is no good measure of compliance or adherence to medication. In this study Altman calls for continued monitoring of NOACS. Given the major impact these drugs have on thrombosis management, Thrombosis Journal introduced a special theme series of articles on NOACs , addressing many of the above issues.
6) But it still is not perfect.
Anticoagulant underuse in risk patients is estimated to be up to 40%. Many different considerations are taken into account by clinicians when prescribing these drugs, and this varies considerably between different specialities, as found in this study.
Additionally, hospital admissions for bleeding while on antithrombotic agents is the number one in potentially avoidable hospital admissions related to medication. Thus increased overtreatment is a potential concern when raising awareness of a condition, and so selective prevention in those who are at highest risk is important. This study looks at the efficiency and safety of warfarin use both inside and outside anticoagulation clinics.
Given the world-wide prevalence of these thrombotic diseases, awareness amongst the public and policy makers is essential. Thrombosis in patients admitted to hospital for surgery or major diseases is still frequent in spite of international guidelines advocating the use of thromboprophylaxis. Hospitals need to establish and enforce protocols for monitoring and preventively treating patients at risk. A process that has already been implemented in some hospitals across the UK.
Comments