
Colorectal cysts: A simple model system for testing the efficacy of CAR-T cells against malignancies
Optimal CAR T therapy validation requires a 3-D cellular system that mimics the complex tumour cellular architecture. In a study published in BMC Biotechnology Dillard et al. report the development of colorectal cysts from a single colorectal cell line Caco-2 as simple and reliable tools to validate CAR T-mediated therapy.
CAR T cells are T lymphocytes, genetically engineered to express a Chimeric Antigen Receptor (CAR) on their surface that recognizes CD19 marker on the surface of B lymphocytes and also promotes signalling events that control the activation of lysis. This results in the destruction of the B lymphocyte. Since CD19 is a widespread marker in cancerous B cells, CAR-T cells are being used as an allogenic treatment of B-cell malignancies. The CAR T-mediated immunotherapy for cancer has revolutionized the treatment of ‘liquid tumors’, i.e, haematological, however, it hasn’t been so effective in the treatment of solid tumors, as CAR-T cells are unable to survive in the complex tumour microenvironment and target successfully all the tumor-generating cells.
For this reason, using a two-dimensional (2-D) cellular system, in which CAR-T cells are added in a monolayer of cultured target cancer cells, to validate CAR-T cell functionality and specificity, is inadequate, as the 2-D system does not mimic the challenging 3-D morphology and organization of solid tumors. Moreover, it has been demonstrated that cancer cells acquire a different gene expression profile when cultured in 3-D spheroids compared to 2-D, which may affect their recognition by CAR-T cells.
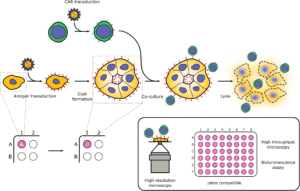
In order to create a simple 3-D cellular system that could be used for the validation of CAR-T cells, the authors took advantage of a colorectal cancer cell line, Caco-2, that has been shown to form 3-D cyst-like structures by self-organisation, with the apical surface of the epithelial cells facing a central lumen. First, they transduced Caco-2 cells with the CD19 gene, in a way that ensured cell-surface expression of the CD19 antigen on their surface (CD19Caco-2 cells). Next, they showed that CD19CAR-T cells were able to kill CD19Caco-2 cells, as effectively as in a 2-D culture, while Caco-2 cells remained intact. Finally, they demonstrated that the system was compatible with super-resolution microscopy, high-throughput live imaging and bioluminescence assays; hence the ability of the CAR-T cells to kill the cancer cells and destroy the cyst can be monitored with both qualitative and quantitative methods.
This is a simple and versatile method that can be adapted to the use of a variety of cancer lines that have been shown to form similar simple 3-D structures. It could therefore, constitute a powerful tool for the therapeutic validation of CAR-T cells in different contexts.
https://doi.org/10.1186/s12896-020-00623-0
Bipolar disease is prevalent in homeless people
Numerous studies have shown that bipolar disease (BD) is a common disorder among homeless people. In a study published in BMC Public Health Ayano et al. performed a systematic review and meta-analysis by pulling existing data from the literature, which confirmed and estimated more accurately the high pooled prevalence of BD among homeless people.
Bipolar disorder (BP) is a mental health condition characterized by lengthy periods of extreme mood swings. BP has a prevalence of about 1-2.4 % in the general population, but has been shown to affect 2.41 to 42.42% of homeless people, depending on the study. BD has a severe negative effect in homeless people and is associated with an increased risk of disability, substance/drug abuse. In order to provide recommendations for future research and clinical practice, the authors performed a systematic review and meta-analysis using the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses) guidelines. From a total of 3236 articles identifies, only 10 articles met the inclusion criteria for the final systematic review and meta-analysis that was conducted. The studies were performed in five countries/continents (Canada, USA, Brazil, Germany, Ireland and France) and were published between 2001 and 2017.
Based on the random-effects model to account for existing heterogeneity the pooled BD prevalence among homeless people was estimated at 11.4%. Subgroup analysis by country/continent showed the prevalence of BD to be 10% in Europe and 13.2 % in other countries, while subgroup analysis by the quality of the studies showed a pooled BD prevalence of 9.9% for high-quality studies and 11.8% for both low and moderate-quality studies. These numbers are significantly higher than the ones reported for the general population.

Likely reasons for this increased between BD and homelessness is the co-occurrence of other medical conditions, such as tuberculosis, HIV/AIDS, which have been associated with an increased risk of bipolar and other mental illnesses. Also, the possible exposure of homeless people to physical and sexual trauma, which is associated with the onset of manic episodes and bipolar disease in risky groups, may also be a factor. Moreover, the higher co-existence of depression, anxiety, psychosis and alcohol-related disorders in homeless people may also constitute a possible reason for the higher prevalence of BD.
This study demonstrates the importance of further high-quality studies to determine the etiologies of the high prevalence of BD observed in homeless people and of targeted interventions to prevent and diagnose BD in these individuals. The authors recommend the strengthening of the mental health services for homeless people.
https://doi.org/10.1186/s12889-020-08819-x
Calculating committed CO2 emissions of the shipping industry
The shipping industry has one of the highest carbon dioxide (CO2) emissions and needs to take action to reduce such emissions as soon as possible. In a study published in BMC Energy Bullock et al. analyses for the first time the committed emissions of the shipping sector taking into consideration individual ship type data from existing and new ships and assesses which measures should be taken to reduce baseline committed emissions to meet the Paris agreement goals for action on climate change.
The United Nations Framework Convention on Climate Change (UNFCCC) Paris agreement goal is to keep the increase of global temperature below 2oC above pre-industrial levels and to pursue efforts to keep the temperature rise below 1.5 oC. For this to be achieved global CO2 emissions need to be reduced as soon as possible.
The shipping sector is the main contributor of CO2 emissions, estimated at around 800 MtCO2 per year, hence it has set a target of at least 50% reduction in CO2 emissions by 2050 compared to 2008. However, until now the committed emissions of shipping, i.e., the CO2 emissions expected based on existing energy infrastructure, are based on assumptions of ship lifetimes extrapolated from other transport systems. The average scrappage age of ships is 28 years, which is much higher than road transport vehicles, therefore, this practice underestimates committed emissions in shipping. As a result, the ‘carbon budget’, which is the amount of CO2 that can be emitted over time while limiting global warming to the accepted levels of the Paris agreement for shipping industry is estimated to be higher for the shipping industry, than it really should.
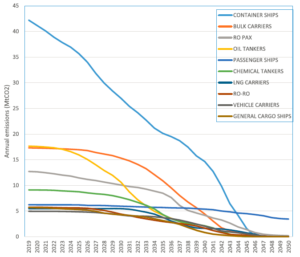
In this study the authors analysed committed emissions in 11,000 existing and new ships in the European Union’s new emissions monitoring scheme (EU MRV), taking into account the wide range of ship types, as well as their different sizes and scrappage age, using datasets published for the first time in 2019. It was found that five ship types: container, bulk carriers, ro pax, oil tankers and passenger ships are responsible for 71% of committed emissions, with the highest baseline committed emissions estimated for container ships. In particular, the new containers account for the highest committed emissions, as although they are more efficient, they are much larger than older containers and this has a greater impact. Moreover, passenger ships were found to have disproportionately high emissions, despite their small numbers, due to their long life time. Overall the baseline committed emissions from all existing ships in the EU MRV fleet was found to be 2260 MtCO2, much larger than estimated in previous studies. This is equivalent to 85-212% of the carbon budget to achieve the 1.5 oC target that is available for the EU MRV fleet, therefore, significant mitigation measures are required to reduce these figures.
The authors found that the combination of four measures: slow speed, technical and operational improvements, fuel blending and the use of zero-carbon fuel, if implemented between 2020s-2030s has the potential to reduce the baseline committed emissions by 65% to 793 MtCO2 and achieve the target of keeping within the Paris agreement carbon budgets, without the need for premature scrappage. However, any delay in appropriate implementation would result in a reduction of only 13% of committed emissions.
This study demonstrates that we cannot rely on measures to improve the efficiency of new ships in order to deliver what is decided in the Paris agreement and highlights the need to implement measures on existing ships, as soon as possible.
https://doi.org/10.1186/s42500-020-00015-2
Pilot study finds: Modified short-term fasting reduces chemotherapy toxicity in gynaecological cancer patients
Chemotherapy-induced toxicity results in patients postponing chemotherapy or in the reduction of the drugs dose used, thus compromising therapy. There’s a lot of evidence to suggest that short-term fasting prior to the onset of chemotherapy has beneficial effects in tolerating chemotherapy. In study published in BMC Cancer Zorn at al. report a significant reduction of toxicity-related symptoms in patients with gynecological cancer, achieved in a controlled cross-over pilot study that used a modified short-term fasting (mSTF) protocol.
Toxicity is a common side effect of chemotherapy, a consequence of healthy cells being destroyed together with the cancer cells by the drug cocktail. Fasting is believed to protect normal cells from the detrimental effects of chemotherapy, as they enter a state of reduced cell division and stress resistance, upregulation of DNA repair and induced autophagy. In tumor cells on the other hand, growth pathways remain activated, which renders them more sensitive to chemotherapy.
In a case series study human patients under various fasting regimens were reported to show significantly fewer toxicity-induced symptoms, such as fatigue, vomiting and diarrhea, while a randomized control trial showed that a 48-h fasting reduced bone marrow toxicity and DNA damage in peripheral blood mononuclear cells. Moreover, a dose-escalation fasting study demonstrated that 72h fasting during chemotherapy was safe and tolerated by the patients, while it resulted in reduced chemotherapy-related toxicity and low-grade fasting-related toxicity.
In this pilot study the authors evaluated the effect of a 96-h fasting on the chemotherapy-induced toxicity in women with gynecological cancer. For the first time the effect of a 6-day intervention of Ketone diet (KD) prior to mSTF on ameliorating the negative effects of fasting was also assessed. The mSTF itself had a ketogenic composition (75% fat, 15% protein and 10% carbohydrate), as it has been shown that fasting achieves best results in a state of ketosis (elevated levels of ketone bodies in the blood). The patients, who underwent a calorie restriction to 25% of their daily requirement, as a result of mSTF tolerated the fasting well and experienced much less severe symptoms of chemotherapy-induced toxicity: significantly fewer patients suffered from stomatitis, headaches and weakness and patients also showed significantly less haematological parameters of toxicity during mSTF cycles. Although previous studies had reported reduced cases of nausea, vomiting and diarrhea after STF, in this particular study, this was not observed, possibly because the patients had already overcome these conditions due to preventive medication. Importantly, the patients on mSTM postponed much fewer chemotherapy appointments than the ones on normal diet, which reflects their better tolerance of their treatment and physical condition in general. It was also found that the KD neither reduced fasting-related discomfort nor improved compliance of the fasting regimen.
These results clearly show the potential of mSTF in counteracting chemotherapy-related toxicity and enhancing tolerance of treatment. Further larger randomized controlled trials are needed to confirm the efficacy of mSTF as a supportive approach to chemotherapy, before recommending this treatment to cancer patients.
https://doi.org/10.1186/s12885-020-07041-7

Comments